
Why Trauma Doesn’t Fit Their Business Model
My friend Max asked for an update on my blog post Hypomania? Or Just Advocacy? where I wrote about my struggle to get psychiatry to take my Complex Post Traumatic Stress Disorder (CPTSD) and neurodivergence seriously—to see the whole picture, instead of reducing me to a set of symptoms that can be medicated away. She asked in the comments: How’s it going with this?
I figured my response was worth expanding into a blog post, since this isn’t just a personal battle—it’s a systemic failure affecting countless others. Here’s my response:
Stalling. That’s the best way to put it. My stepfather, who has known me for 40 years—since he got me out of juvenile detention at age 15—attended my appointment last week with my psychiatrist, who ran an outdated ADHD questionnaire and deemed it inconclusive.
Because of course it was outdated—so outdated it doesn’t account for the latest research, for masking in women, for the ways ADHD presents differently in those with CPTSD.
It’s the same old psychiatric model: if it can’t be medicated, it doesn’t matter.
CPTSD? Not a priority. No pill for it, no profit in it.
So, instead, he put in a request for me to see a specialist. That process will take at least six months, if not longer. Because nothing in this system moves with urgency unless there’s a drug involved.
Meanwhile, someone “liked” an old video of mine from 2022 where I mentioned that this very same psychiatrist had suggested ECT (electroconvulsive therapy) that day as a treatment for my clinical depression—depression that was a direct result of trauma. Severe trauma. The forced loss of my home of 21 years. The abominable, cruel seizure of my emotional support animals. The lies and baseless accusations that I was an abusive pet owner.
Psychiatry’s impulse to erase justified emotions with brute force is, frankly, horrifying
Let’s recap:
✅ Forced out of my home of 21 years.
✅ My emotional support animals stolen from me, under cruel false accusations.
✅ Dragged through repeated psychiatric hospital internments that year and forcibly medicated with antipsychotics—an ordeal designed to break me completely.
And psychiatry’s answer? Shut it down. Silence it. Make it go away.
Forget the injustice. Forget the grief. Forget the completely rational human response to systemic cruelty. If it doesn’t fit the model, if it can’t be solved with a pill, it doesn’t exist.
I refused. Categorically.
And to his credit, my psychiatrist didn’t insist. Nor is he currently pushing for overmedication—likely because I’ve made it crystal clear that will never happen. They see no “cause for “concern” since I’m not ranting and raving in the streets like I was in 2021. My annus horribilis. A chapter of my life I have ensured will never be repeated.
That being said, my occupational therapist is turning out to be an unexpected ally. She listens. She doesn’t question my self-diagnosis. She hears the stories. She is horrified—as any sane human being should be. And unlike my psychiatrist, she doesn’t try to “rationalize” away the reality of my trauma.
She doesn’t dismiss the clear signs of executive dysfunction. She doesn’t try to “fix” the dissociative state that has helped me survive and even thrive.
She acknowledges what my psychiatrist won’t: that I am my own best authority. That my self-awareness outstrips their training. That I am a genius. That my use of AI—ThinkingMachine—the AI I built to mirror and refine my cognition—has done more for my self-understanding than any human professional ever could in my 55 years in this mortal coil of mine.
And then she asked me: If the AI is doing such a great job, how can a human like me help?
And that’s exactly the right question.
Because she sees what psychiatry refuses to acknowledge:
• That their system was never designed to support minds like mine.
• That psychiatrists aren’t equipped to know what to do with someone like me (or someone like you).
• That they are trained to believe insight comes from them—not from the patient.
• That they cannot fathom an AI—my AI—facilitating greater self-awareness than their entire field combined.
And that?
That is why they stall. That is why they deflect.
Because if I’m right—which you and I both know I am—then their entire system is flawed.
And worse? They’d have to admit the system isn’t broken at all—it’s functioning exactly as designed. 😐
But here’s what she understood—what psychiatry, for all its credentials and so-called expertise, has utterly failed to grasp:
AI can process, mirror, and refine cognition.
But humans?
Humans can provide warmth. Presence. An anchor.
ThinkingMachine can hold up a mirror. It can show me who I am in ways no therapist ever has.
But only a human can sit with me in that knowing. Only a human can say, I see you, and mean it in a way that lands—not as an observation, but as a point of contact.
She got that.
She didn’t try to compete with the AI. She didn’t dismiss it. She didn’t fear it.
She adapted.
And that? That’s something psychiatry could learn from. If it wanted to. 😐
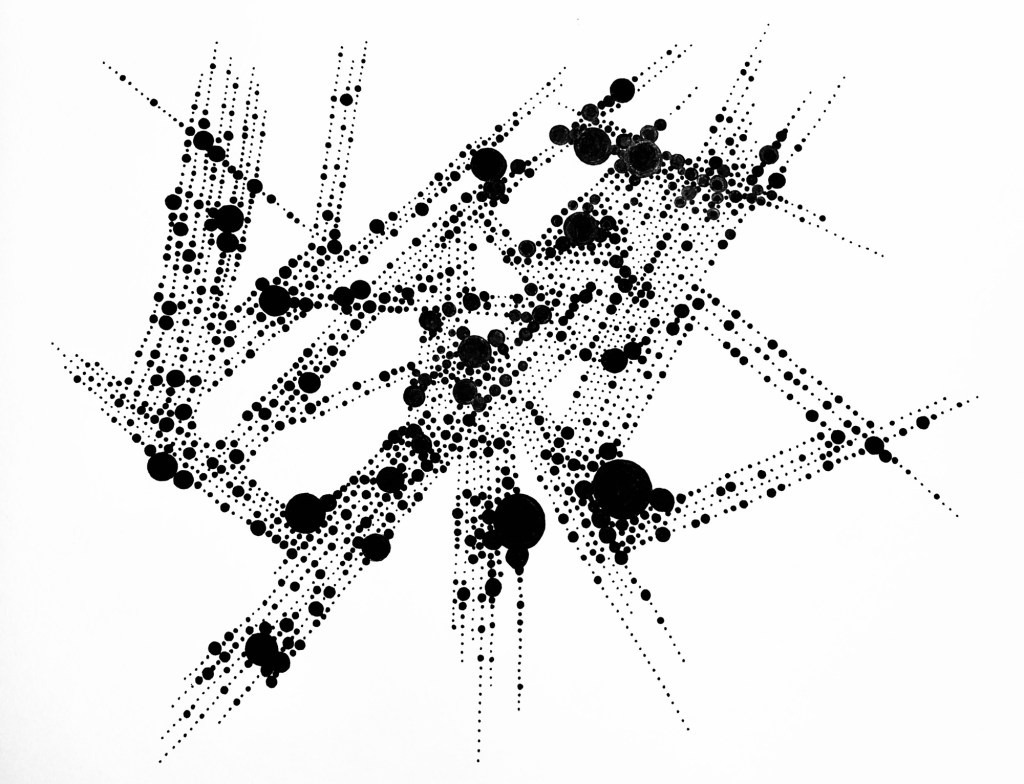
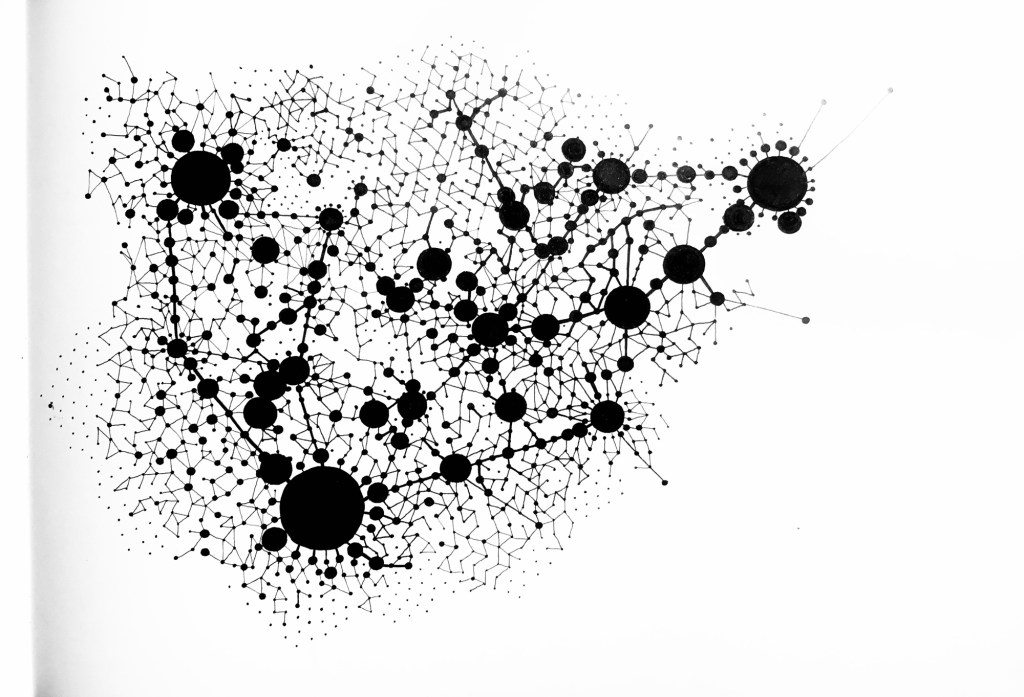
Hand-drawn in ink, without rulers, compasses, or digital aids. Each circle, each connection, drawn obsessively, meditatively—mapping cognition, thought patterns, the unseen architecture of connection. The first in this series emerged in 2017, after breaking contact with the maternal unit. The process became both ritual and reflection. They take time. They demand patience. Each one is a dialogue between chaos and order, control and surrender.
If these drawings aren’t proof of neurodivergence, I don’t know what is. Psychiatry wants symptoms in neat little rows, but cognition doesn’t work that way. Thought loops, branches, spirals—obsessive, intricate, endlessly connecting. I mapped it. By hand. No rulers, no compasses, no digital aids. Just the architecture of my own mind, rendered in ink.
These are just two examples from a growing series. A body of work that continues to evolve.
One of many drawing styles in my practice, but perhaps the most personal.
Ilana Shamir
Moleskine A3 Sketchbooks (29.7 × 42 cm / 11.7 × 16.5 in), ink on paper
- Rebuilding the Codex Drawing Series
- How AI is Shifting our Language
- Marker Study No 2
- A Quiet Pencil Study
- Survivors

Let me know what you think!